Appendix C - Glossary for Clinical Assessment
This section aims to provide criteria, definitions, and examples to calibrate learner evaluation using the UNC Adams School of Dentistry Assessment for Clinical Encounter (ACE). The clinical assessment process is based on the Entrustable Professional Activity (EPA) framework and the ADEA Compendium of Clinical Competency Assessment.
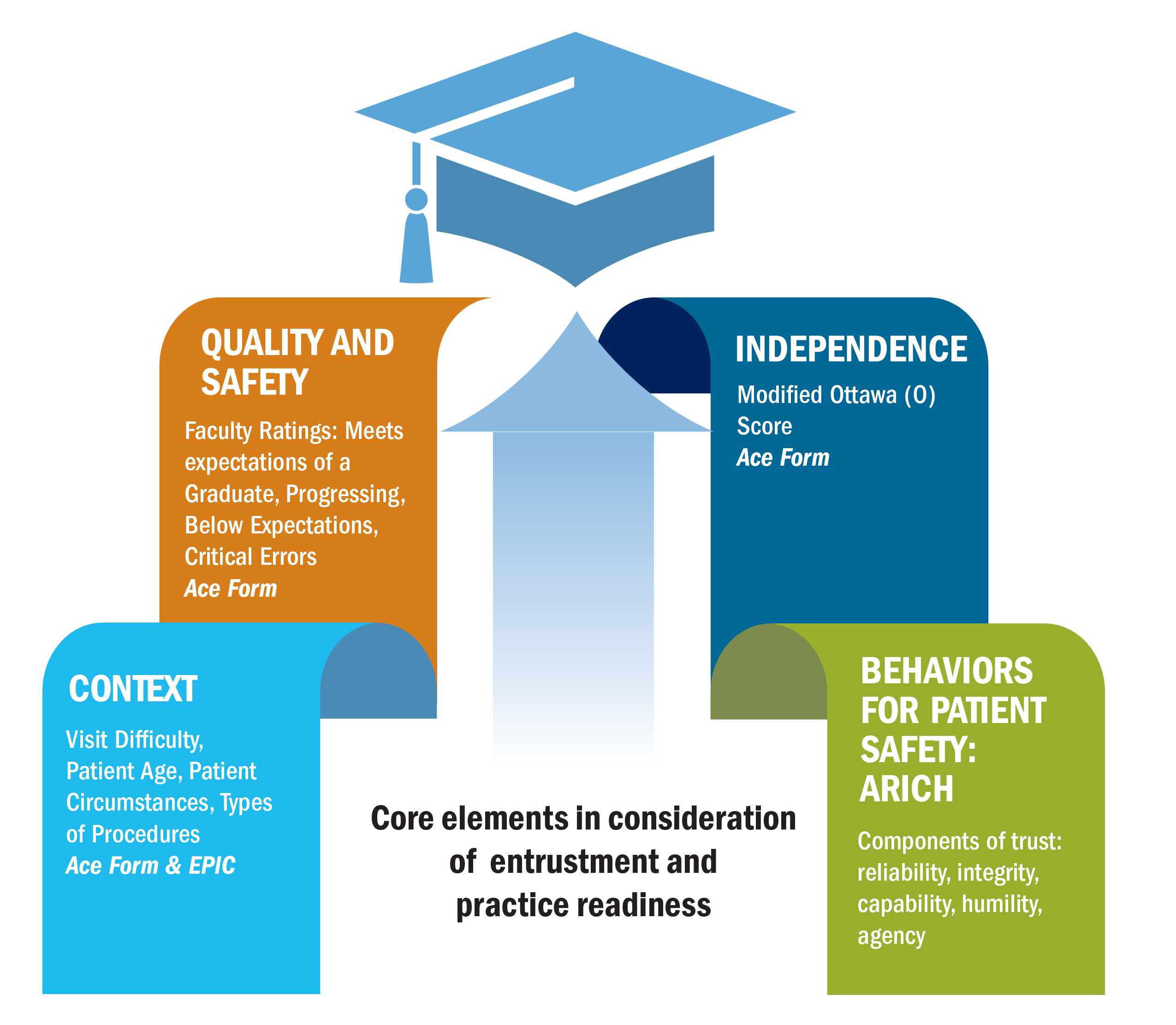
Quality
Ratings to assess quality as defined by the Adams School of Dentistry:
- Meets expectations of the graduate: Has met standards for practice readiness.
- Progressing: Developing skills appropriate for learners’ level (DDS2/DDS3/DDS4).
- Below expectations: Performing at a substandard level that may or may not include a critical error
Critical Errors
Definition: An event or unprofessional behavior that disrupts safe, legal, and ethical person-centered care. A critical error includes events or behaviors — whether evident or harmful to the patient — that could lead to, but not limited to, disciplinary action by an employer or Board of Dentistry. In an academic setting, repeat critical errors may prompt discussions for dismissal from the program.
| Domain | Critical Errors |
| Advocate |
|
| Clinician |
|
| Thinker |
|
Independence
Independence ratings are based on the Ottawa Surgical Competency Operating Room Evaluation (O-SCORE), designed to assess a learner’s level of independence using behavioral anchors.
1. Retrospective O-SCORE:
How much supervision did the learner need during the entire encounter?
- Faculty had to do it for the learner (hands-on intervention)
- Faculty had to talk the learner through it (consistent verbal guidance)
- Faculty had to prompt the learner from time to time (intermittent verbal guidance)
- Faculty did not have to direct or intervene (procedure completed independently)
2. Prospective O-SCORE:
How much supervision should the learner have on a future encounter that is similar?
- Faculty would have to do it for the learner (hands-on intervention)
- Faculty would have to talk the learner through it (consistent verbal guidance)
- Faculty would have to prompt the learner from time to time (intermittent verbal guidance)
- Faculty would not have to direct or intervene (procedure completed independently)
- Faculty would not need to be there (independence)
Context
Visit Difficulty, Patient Age, Patient Circumstances, Types of Procedures
| Criteria | Definition |
| Visit Difficulty |
|
| Patient Age |
|
| Patient Circumstances (Follows CODA Standard 2-25) |
|
ARICH
This framework reflects key behaviors for patient safety and quality care, including agency, reliability, integrity, capability and humility described earlier in this document.